Almost all modern technologies and medical solutions are presented as neutral and universally applicable. “One size fits all.” In reality, the experience of women all over the world shows that these systems have been developed using men as the default human subject. Everyday necessities, from cars to toothpaste, have been designed and tested with the male body and biology in mind, disregarding that of women. Because data drawn from male bodies and male experiences has long been treated as the standard for all people when it comes to product design and medical development, women are frequently left with no choice but to use products and treatments that are less effective, less safe, or unsuited for their physiology.
This phenomenon is documented across engineering standards, clinical trial data, regulatory history, and peer-reviewed research. Examining how these medical and design-based biases arose and how they continue to shape the lives of women reveals a fundamental problem in a great multitude of industries: their roots stretch deep into soil tainted with misogyny, sexism, and a historical disregard of women’s needs.

How Bias Became Built In
In the past, scientific and medical research has largely considered only male subjects. Throughout the 20th century, women have been excluded from clinical trials. The exclusion was made official in the United States during 1977, when the Food and Drug Administration recommended not including women of childbearing potential in early-phase drug trials due to concerns about hormones and fetal risk (Medidata, history of women in clinical trials). This policy had lasting consequences. Even after the 1993 National Institute of Health Revitalization Act required the inclusion of women in federally funded research, many trials continued to enroll disproportionately male participants or failed to analyze results by sex (AAMC). In addition, leading products like Tylenol and Ibuprofen were already patented, sold widely in stores, and in clinical use before this act, meaning that their formulas had already been cemented and would remain unaffected by the act’s requirements. As a result, male physiology became the industry standard for understanding disease progression and treatment.
Industrial design followed suit in this pattern. Anthropometric datasets used to set product dimensions and safety standards were derived from male populations, those being mainly military personnel and industrial workers. These measurements became the standard of future design, making the bodies of male workers the blueprint for products meant for a diverse range of bodies (Criado Perez, Invisible Women).
Everyday Products and Systems Designed for Men
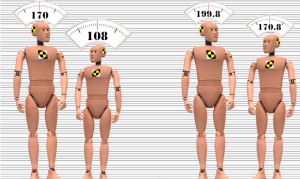
One of the best documented examples of male-centered design is vehicle safety. For decades, automobile crash testing relied almost exclusively on crash test dummies modeled based on the average male. These dummies were 5 feet 9 inches tall and weighed around 170 pounds (Consumer Reports). At the time, this was accurate to the male body’s shape and weight. Female dummies, if used at all, were often just scaled-down versions of male models and not anatomically accurate models of the female body.
Research cited by Consumer Reports shows that women are 73% more likely than men to be seriously injured in a frontal car crash and 17% more likely to die in one. These differences are caused by variations in neck strength and torso shape between females and males, neither of which were adequately accounted for in the testing of vehicles.
Beyond automobiles, everyday products are also derived from male-centered research and trials. Tools and safety equipment are frequently designed using male hand sizes and grip strength as guidelines (Monash University Accident Research Centre). Poorly fitting equipment increases the risk of injury, particularly in industrial and medical settings, yet women are expected to adapt to these design flaws rather than them being revised with their bodily differences from men being considered.
Medical Research
The consequences of male-centric research are especially severe in medicine. A significant proportion of drugs currently on the market were approved based on clinical trials that enrolled mostly male participants. According to reviews published in Applied Clinical Trials, sex-based differences in drug absorption were often discovered only after widespread use, when debilitating effects in large groups of women became clear.
Women generally have different enzyme activity and fluctuating hormone levels, both of which can affect how drugs are absorbed and processed. Failure to account for these differences has led to higher rates of adverse drug reactions among women. The U.S. Government Accountability Office has reported that several drugs withdrawn from the market posed greater health risks for women than men, these risks not being detected during pre-approval trials.
Diagnostic bias further develops this issue. Cardiovascular disease, the leading cause of death among women in the United States, was long studied primarily in male subjects. As a result, medical education for future nurses and doctors emphasized male-typical symptoms such as chest pain, while symptoms seen more often in women, including fatigue and nausea, were acknowledged less. This led to delayed diagnoses and worse outcomes for women experiencing cardiovascular disease.
Biased Funding for Research
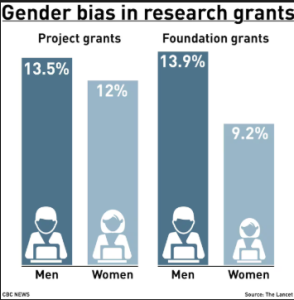
Gender bias also shapes which health issues receive funding and sustained research attention. Conditions that primarily impact women are often underfunded when it comes to their severity. Autoimmune diseases, which disproportionately affect women, remain poorly researched despite their chronic and sometimes disabling nature.
In contrast, male-pattern baldness has received extensive pharmaceutical investment. Although hair loss poses no threat to physical health and mortality, it has attracted decades of research and solution development. Scholars and commentators have noted this disparity as representative of how market incentives and priorities favor male concerns, even though women’s health concerns tend to be more often fatal. Publication bias supports these trends. A study documented in PubMed found that research involving male subjects was more likely to be recommended for publication than similar studies involving female subjects, skewing which findings enter the scientific canon and inform future research.
Consequences for Women’s Health and Safety
The impact of these biases over time is measurable. Women experience greater injury risk from safety systems and delays in diagnosis for life-threatening conditions. These outcomes are the result of systemic choices about who is studied, whose data is collected, and which problems are deemed worthy of investigation by the market’s interests.
Because male-centered data is treated as neutral, the harm they produce is often individualized. Women are told that their symptoms are atypical or that adverse reactions are unfortunate but rare. This response, shaped by years of women being disregarded in the research industry, distracts from the origins of the problem and avoids accountability.
Addressing these disparities requires institutional change. Clinical trials must include adequate amounts of female subjects and analyze outcomes with regard to sex, instead of relying on generalizations. Design standards must be revised using inclusive anthropometric data rather than treating male bodies as the default model of all bodies. Research funding must align with disease burden instead of public appeal alone. Regulatory agencies and advocacy organizations have begun to push for these changes, but progress remains inconsistent. Recognizing that “gender-neutral” has often meant “for men” by default is a necessary step toward systems that genuinely serve the whole population.